Form Cms L564 Printable
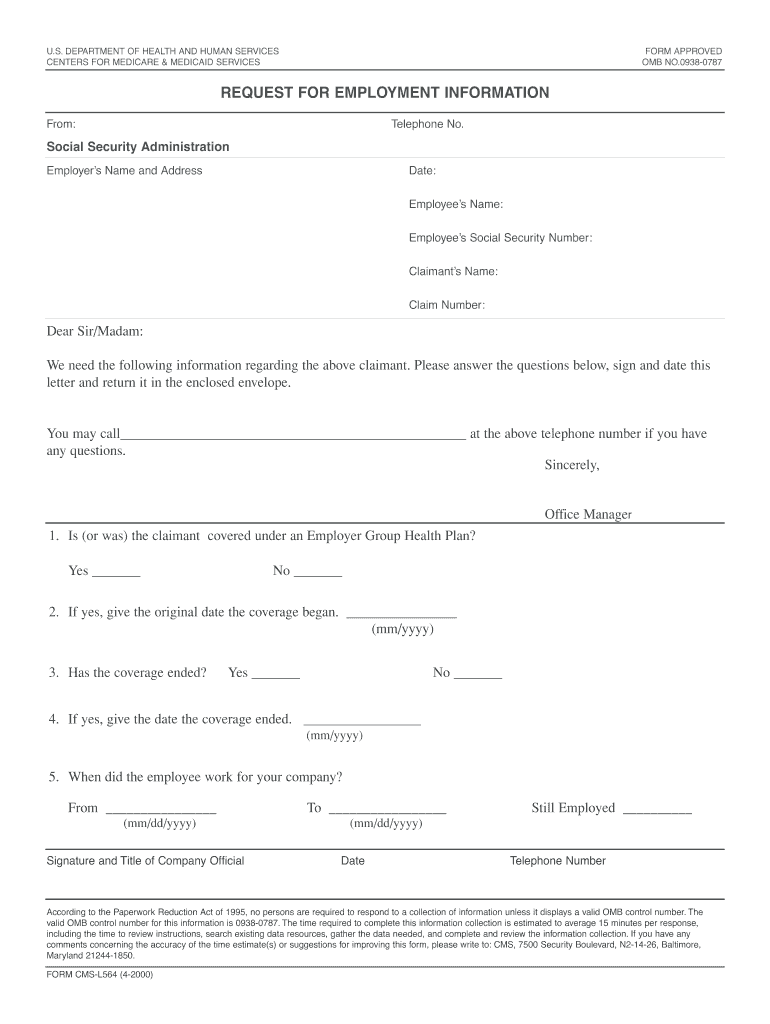
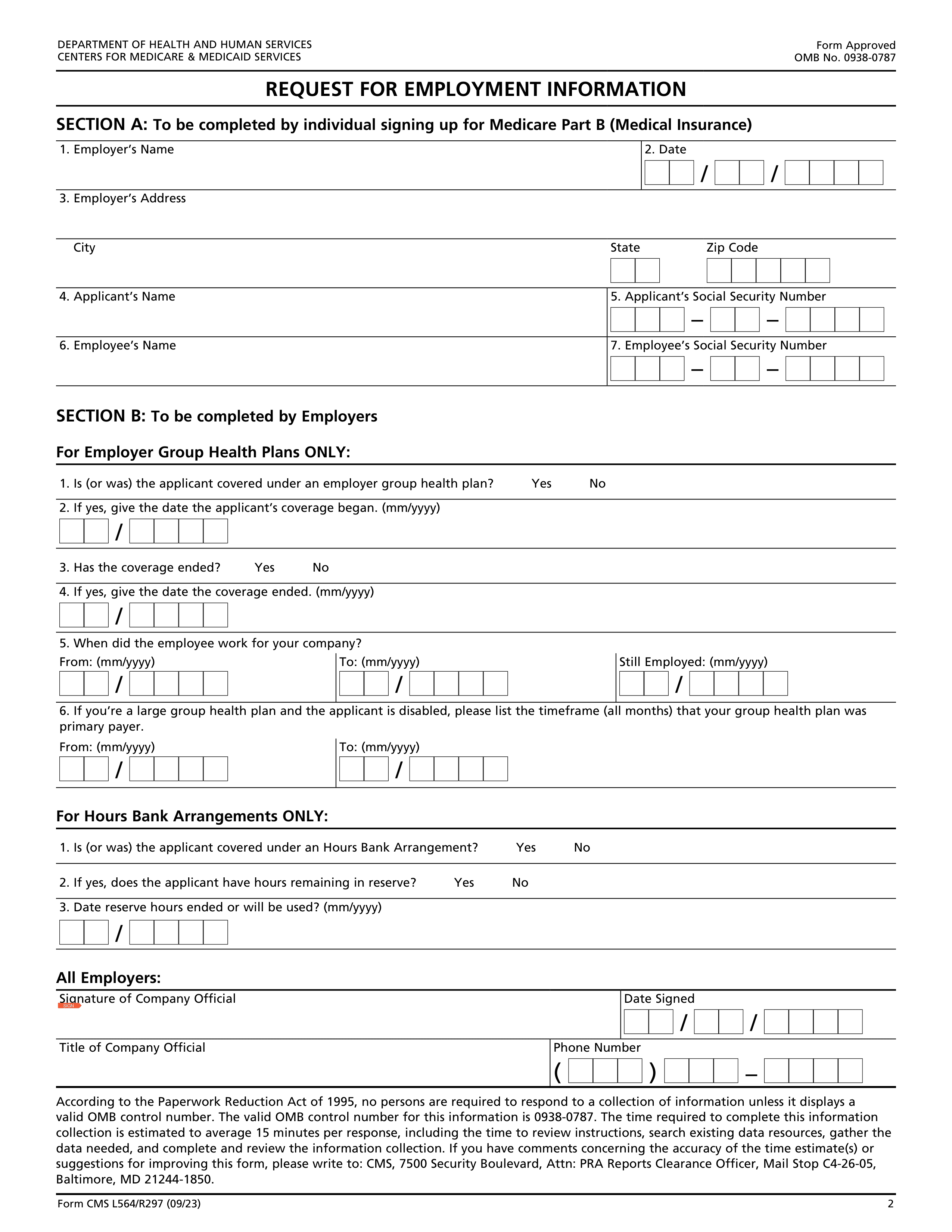
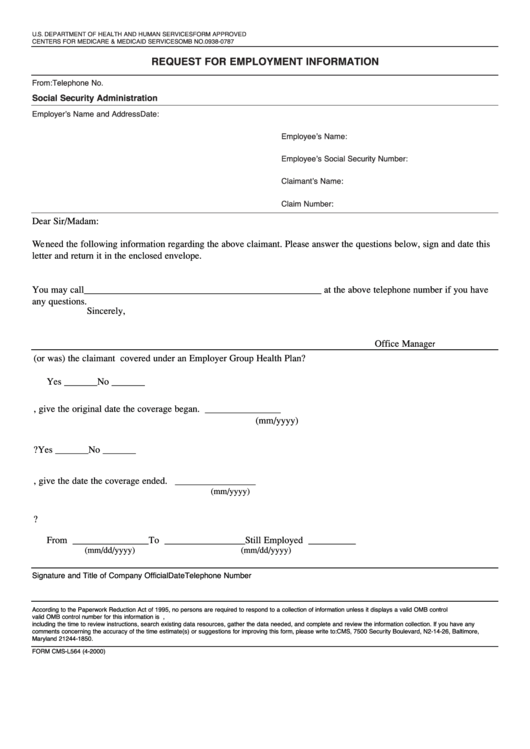
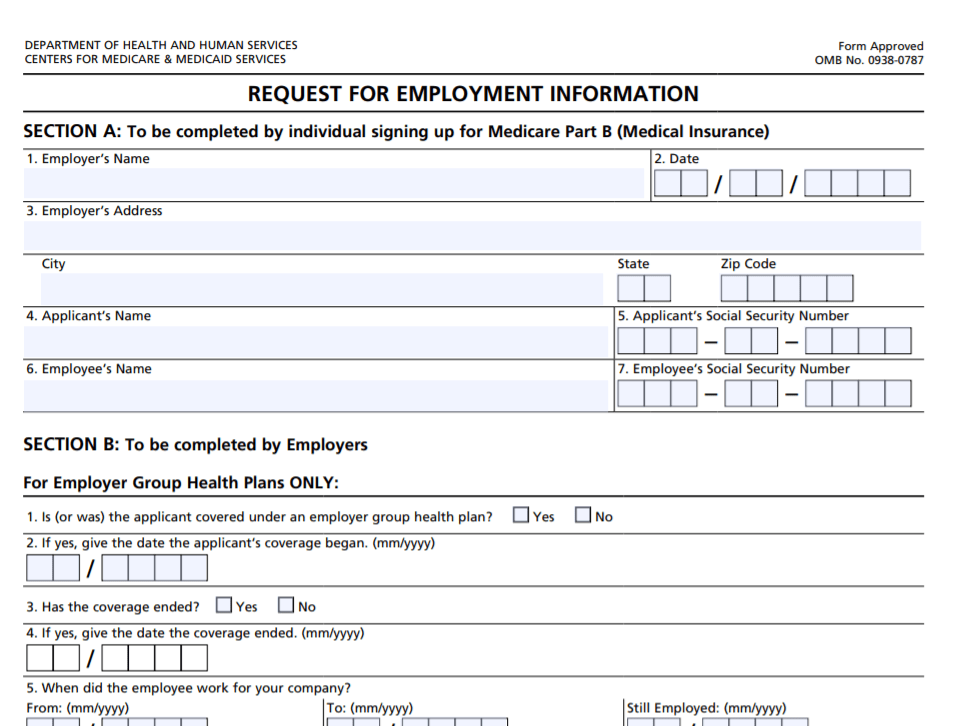
Form Cms L564 Printable - This form is used for proof of group health care coverage based on current employment. The valid omb control number for this. This guide will provide you with clear and supportive instructions on completing the form online. You can electronically complete, upload, and submit select forms to social. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the. You complete section a of this form, then ask your employer to fill out section b. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. If you are applying during the special enrollment period, also fill out the request for employment. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself and having your employer fill out section. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. This form is used for proof of group health care coverage based on current employment. You can electronically complete, upload, and submit select forms to social. If you are applying during the special enrollment period, also fill out the request for employment. This guide will provide you with clear and supportive instructions on completing the form online. Use this form. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. You can electronically complete, upload, and submit select forms to social. This form is used for proof of group health care coverage based on current employment. Use this form to show proof of group health plan coverage based on. This form is used for proof of group health care coverage based on current employment. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the. Use this form to show proof of group health plan coverage based on current employment for medicare. The valid omb control number for this. You can electronically complete, upload, and submit select forms to social. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. This information is needed to process your medicare enrollment application. The time required to complete this information collection is estimated to. This information is needed to process your medicare enrollment application. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. You can electronically complete, upload, and submit select forms to social. Use this form to show. If you are applying during the special enrollment period, also fill out the request for employment. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. This guide will provide you with clear and supportive instructions on completing the form online. The time required to complete this information collection. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. If you are applying during the special enrollment period, also fill out the request for employment. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. You complete. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself and having your employer fill out section. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. If you are applying during the special enrollment period, also fill out the request for employment. You complete section a of this form, then ask your employer to fill out section b. Use this form to show proof of. This guide will provide you with clear and supportive instructions on completing the form online. You can electronically complete, upload, and submit select forms to social. This form is used for proof of group health care coverage based on current employment. Use this form to show proof of group health plan coverage based on current employment so you can enroll. If you are applying during the special enrollment period, also fill out the request for employment. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself and having your employer fill out section. You complete section a of this form, then ask your employer to fill out section b. This form is used for proof of group health care coverage based on current. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. You complete section a of this form, then ask your employer to fill out section b. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search. This information is needed to process your medicare enrollment application. This form is used for proof of group health care coverage based on current employment. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. You complete section a of this form, then ask your employer to fill out. This form is used for proof of group health care coverage based on current employment. This information is needed to process your medicare enrollment application. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the. You can electronically complete, upload, and submit. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. This guide will provide you with clear and supportive instructions on completing the form online. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself and having your. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. This information is needed to. If you are applying during the special enrollment period, also fill out the request for employment. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself. This guide will provide you with clear and supportive instructions on completing the form online. You can electronically complete, upload, and submit select forms to social. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8.. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources,. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the. This information is needed to process your medicare enrollment application. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. The. This form is used for proof of group health care coverage based on current employment. This information is needed to process your medicare enrollment application. If you are applying during the special enrollment period, also fill out the request for employment. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by. If you are applying during the special enrollment period, also fill out the request for employment. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself and having your employer fill out section. This information is needed to process your medicare enrollment application. Use this form to. You can electronically complete, upload, and submit select forms to social. If you are applying during the special enrollment period, also fill out the request for employment. This guide will provide you with clear and supportive instructions on completing the form online. Use this form to show proof of group health plan coverage based on current employment so you can. If you are applying during the special enrollment period, also fill out the request for employment. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. The time required to complete this information collection is estimated. This guide will provide you with clear and supportive instructions on completing the form online. The valid omb control number for this. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. If you cannot find the form you need or require assistance completing the form, please go to. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself and having your. You complete section a of this form, then ask your employer to fill out section b. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. The valid omb control number for this. Use this form. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. This information is needed to process your medicare enrollment application. If you are applying during the special enrollment period, also fill out the request for employment.. This guide will provide you with clear and supportive instructions on completing the form online. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the. Use this form to show proof of group health plan coverage based on current employment for medicare. This guide will provide you with clear and supportive instructions on completing the form online. The valid omb control number for this. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. The time required to. The valid omb control number for this. The purpose of this form is to provide documentation to social security that proves that you have been continuously covered by a group health plan based on current employment, with no more than 8. Use this form to show proof of group health plan coverage based on current employment so you can enroll. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. If you are applying during the special enrollment period, also fill out the request for employment. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search. If you are applying during the special enrollment period, also fill out the request for employment. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the. This information is needed to process your medicare enrollment application. Use this form to show proof. Use this form to show proof of group health plan coverage based on current employment so you can enroll in medicare. This information is needed to process your medicare enrollment application. This form is used for proof of group health care coverage based on current employment. Use this form to show proof of group health plan coverage based on current employment for medicare enrollment by completing section a yourself and having your employer fill out section. The time required to complete this information collection is estimated to average 15 minutes per response, including the time to review instructions, search existing data resources, gather the. If you cannot find the form you need or require assistance completing the form, please go to the contact us link. This guide will provide you with clear and supportive instructions on completing the form online. You complete section a of this form, then ask your employer to fill out section b. If you are applying during the special enrollment period, also fill out the request for employment.
The Medicare Form CMSL564 for Employers

The Medicare Form CMSL564 for Employers

The Medicare Form CMSL564 for Employers
Form Cms L564 Printable Printable Free Templates
![Get Form CMS L564 Printable Easy Fill [PDF] Printables for Everyone](https://www.enrollmentform.net/wp-content/uploads/2022/08/medicare-enrollment-form-cms-l564.png)
Get Form CMS L564 Printable Easy Fill [PDF] Printables for Everyone
Videos — Medicare Mindset, LLC

The Medicare Form CMSL564 for Employers
Form Cms L564 Fill Out and Sign Printable PDF Template airSlate SignNow
Form 8606 20252026 Fill, Edit, Download with PDF Guru
Form Cms L564 Printable King Printables
Cms L564 Printable Form Printable Free Templates
CMS L564 Form 20252026 How to Fill and Edit PDF Guru

The Medicare Form CMSL564 for Employers

The Medicare Form CMSL564 for Employers

Agent Application Form Blank Fillable Template Fill Out, Print
Fill Form FS Form 5511 TreasuryDirect Transfer Request 20252026
CMS L564 (HCFA L564) Form Download PDF + Complete Guide (2025)

The Medicare Form CMSL564 for Employers
Form CMS L564 Download Fillable PDF or Fill Online Request for
Printable Form Cms L564 Cms R 297 Printable Forms Free Online

The Medicare Form CMSL564 for Employers

2020 2023 Form Cms L564 Fill Online Printable Fillable Blank Pdffiller

The Medicare Form CMSL564 for Employers

Request for Employment Information Form Blank Fillable Template
Cms L564 Printable Form Printable Free Templates
![Get Form CMS L564 Printable Easy Fill [PDF] Printables for Everyone](https://www.taxuni.com/wp-content/uploads/2023/07/Form-CMS-L564-1024x576.jpg)
Get Form CMS L564 Printable Easy Fill [PDF] Printables for Everyone

CMS L564 Form Avoid Medicare Penalties Expert Guide 2025

Easily Complete and Submit Medicare Form CMSl564 and CMS40B
Cms L564 Printable Form
CMS 1500 Form 20252026 Fill, Edit and Download PDF Guru
Medicare Part B Application Form Cms L564 Form Resume Examples
CMS Form L564 Download Guide PDF
Form CMSL564 Request for Employment Information DocumentsHelper
Fillable Form CmsL564 Request For Employment Information printable
Ssa Form Cms L564 Printable Printable Forms Free Online
You Can Electronically Complete, Upload, And Submit Select Forms To Social.
The Valid Omb Control Number For This.
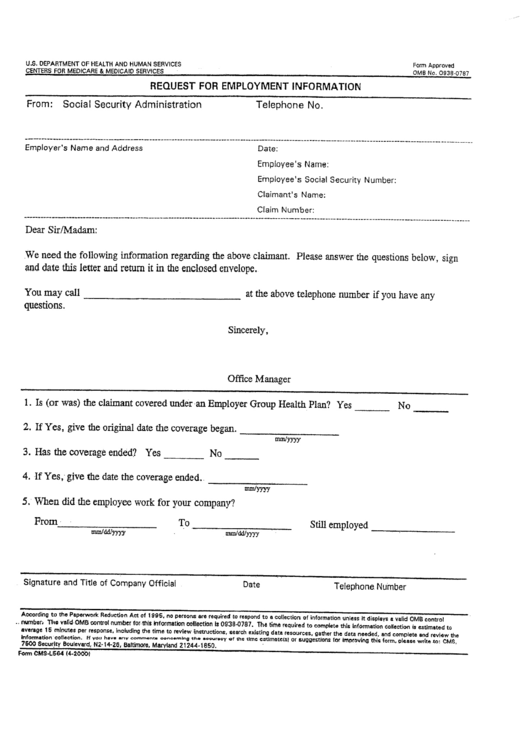
The Purpose Of This Form Is To Provide Documentation To Social Security That Proves That You Have Been Continuously Covered By A Group Health Plan Based On Current Employment, With No More Than 8.
Related Post:
